
-
Historical Perspective, Epidemiology, and Methodology
-
Overview of the SCD guidelines and chapters
-
Process and methodology
-
Consensus Statements
-
Clinical Practice Guidelines and the institute of Medicine
-
Prevention of invasive infection
-
Screening for Renal Disease
-
Electrocardiogram Screening
-
Screening for hypertension
-
Screening for Retinopathy
-
Screening for risk of stroke using neuroimaging
-
Screening for Pulmonary disease
-
Reproductive counseling
-
Contraception
-
Clinical Preventive services
-
Immunizations
-
Vaso-Occlusive Crisis
-
Fever
-
Acute Renal Failure
-
Priapism
-
Hepatobiliary Complications
-
Acute Anemia
-
Splenic Sequestration
-
Acute Chest Syndrome
-
Acute Stroke
-
Multisystem Organ Failure
-
Acute Ocular Conditions
-
Chronic pain
-
Avascular Necrosis
-
Leg Ulcers
-
Pulmonary Hypertension
-
Renal Complications
-
Stuttering/Recurrent Priapism
-
Ophthalmologic Complications
-
Summary of the Evidence
-
Hydroxurea Treatment Recommendations
-
Consensus Treatment Protocol and Technical remarks for the implementation of Hydroxyurea Therapy
-
Indications for transfusions
-
Recommendations for Acute and Chronic Transfusion Therapy
-
Appropriate Management/ Monitoring
-
Consensus Protocol for Monitoring Individuals on Chronic Transfusion Therapy
-
Complications of Transfusions
-
Recommendations for the Management and Prevention of Transfusion Complications
-
New Research is Needed
-
Data Systems That Meet the Highest Standards of Scientific Rigor Can Be Invaluable
-
Improved Phenotyping is needed
-
Broad collaborations for Research and Care
-
Beyond Efficacy
-
Look, Listen, Empathize and Ask
Participants 225


Background
Avascular necrosis (AVN, also known as aseptic necrosis, osteonecrosis, or ischemic necrosis) is bone death due to compromised blood supply. Necrosis can occur when capillaries are occluded by sickled erythrocytes at distal portions of a bone near a joint where hypoxia is maximal and collateral circulation is inadequate. The hip joint is the most common site of AVN. Involvement of the shoulder and other joints is less common. Risk factors for AVN of the femoral head include SCD genotype, age, frequency of painful episodes, hemoglobin level, anda-gene deletion. The overall prevalence of AVN in SCD is about 10 percent, whereas in people with hemoglobin SS, it is about 50 percent by age People with HbSS and concomitant a-thalassemia are at particular risk. The SCD genotypes that are associated with relatively mild anemia, such as HbSS-a-thalassemia and HbSf3°-thalassemia, are at a particularly high risk to develop AVN at a younger age.
AVN of the femoral head causes chronic severe pain and disability. The pain is generally worse on walking, relieved by rest, and may be accompanied by a moderate or severe limitation of motion when the patient bears weight on the affected extremity. About 40-80 percent of cases of AVN of the hips are bilateral and, hence, evaluation of patients with AVN should focus on both hips.
The therapeutic approach to AVN depends on the stage of the disease. Ficat proposed a four-stage radiographic classification of AVN of the hip based on plain radiography. MRI was not available at the time. Steinberg et al. expanded the Ficat staging system into six stages using MRI data. A report from the Comprehensive Sickle Cell Centers (CSCC) investigators defined an adaptation from the Ficat and Steinberg systems that combines radiography, MRI, and bone scans. The adaptation is provided below in exhibit 8.
Exhibit 8. Stages of Avascular Necrosis
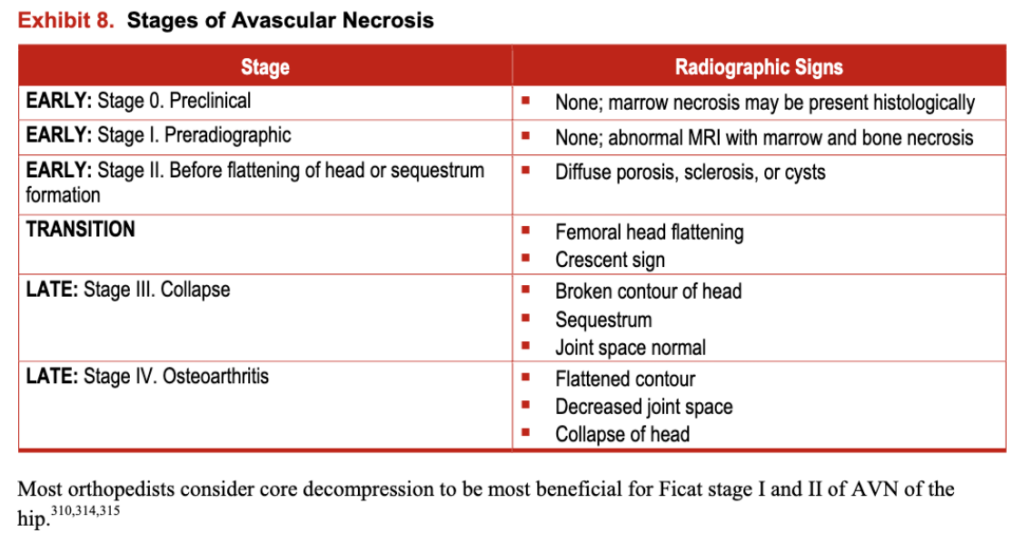
Most orthopedists consider core decompression to be most beneficial for Ficat stage I and II of AVN
Key Question
Summary of the Evidence
The literature review yielded 1 RCT, 16 observational studies, and 16 case reports describing AVN and treatment outcomes. The overall quality of the evidence was low.
The RCT was a randomized prospective multicenter study of 38 adults (81 percent of enrollees), which evaluated the safety of hip core decompression and compared the results of decompression and physical therapy with those of physical therapy alone for the treatment of osteonecrosis of the femoral head in people with all types of SCD. Results showed that physical therapy alone was as effective as hip core decompression followed by physical therapy in improving hip function. However, the evidence provided by this study is limited due to its small sample size and the high attrition rate.
The 16 observational studies and 16 case reports described AVN of various bones in the context of SCD. These studies included more than 350 people (mostly adults) and most commonly reported on people with SCD with AVN of the femoral head. All studies but one were noncomparative, used hip arthroplasty, and reported a high success rate. A few studies reported the use of standard symptomatic therapy with minimal success. In the comparative study,317 the benefit of the surgical intervention (core decompression) in improving pain and evolution of necrotic lesions was significant relative to conservative management.
The methodological quality of the 16 observational studies was low (mainly observational non controlled studies with unclear enrollment criteria). The single comparative study had groups with similar baseline characteristics and outcome ascertainment methods. None of the studies reported adjustment of analyses for confounders.
Recommendations
Evaluate all children and adults with SCD and intermittent or chronic hip pain for AVN by history, physical exam, radiography, and MRI as needed.
(Strong Recommendation, Low-Quality Evidence)
Treat AVN with analgesics and consult physical therapy and orthopedics for assessment and follow up.
(Strong Recommendation, High-Quality Evidence)
Refer symptomatic patients with advanced stages of AVN to an orthopedic surgeon and SCD specialist for evaluation and possible hip arthroplasty.
(Consensus-Panel Expertise)